Pennsylvania Senate Hearing: Large, growing, consistent, compelling body of evidence shows frac’ing negatively impacts public health; PA must act. Ten years later, Health Canada still won’t publicly release their frac hazard study. In Canada, frac panel members lie, ignore evidence; authorities refuse to study cumulative harms; “regulators” like AER refuse to enforce the law while engaging in fraud to serve law-violating polluters (most foreign owned) and further abuse the harmed.
Thank you, Senator. And I thank you all for the opportunity to speak here today.
I’m a professor in the Johns Hopkins Bloomberg School of Public Health. And I’m also appointed as a professor in the Department of Population Health Sciences at Geisinger in Danville, Pennsylvania.
And there at Geisinger, I am the founding director of the Environmental Health Institute, which we founded in 2007. And over the last 15 years, I’ve spent regular time in Danville.
We founded the Environmental Health Institute in 2007. So when this industry and its drilling took off in the late otss, you know, 2009, 2010, we were sort of in the right place at the right time.
And we were charged with evaluating how environmental exposures could be affecting Geisinger’s patients.
I am a physician and an environmental epidemiologist, and I have led many studies of the fracking industry and health at Geisinger.
All of our studies are funded by the National Institutes of Health, which requires rigor and its funded science. And all of our research ideas are subjected to peer review before we’re funded.
I was asked to come here today to talk about the fracking industry and health.
This industry is a large-scale industrial engineering project that involves a number of impacts on communities and their environments.
Ya, they make a lot of money via massive subsidies paid for by taxpayers and the harmed in the USA and Canada and via conning banks, investors and pensions (including AIMCo & Canada Pension Plan Investment Board).
It involves many steps over time, clearing land, building roads, preparing the surface, bringing in chemicals and large volumes of water, bringing in large and heavy equipment like drilling engines and compressor engines.
Then drilling and hydraulic fracturing. Receiving returned liquids and processing them at the surface. Receiving and processing gas at the surface.
Sending the gas through pipelines. And also a disposing of the waste stream.
And this requires monitoring of the safety of all of these steps.
Now, I’m using a shorthand calling this the fracking industry, but that’s really kind of doing a disservice because that’s just one short phase of this multi-phase and long-lasting industry.
Over 10,000 wells are operating in the state. And so this illustrates the huge scale of the impact.
As we think about how this can affect health, we have to think about all these accumulating effects and how this can happen over time.
What Do Communities Experience
Now, what’s a community’s experience?
They experience truck traffic and their diesel exhaust emissions, transient workforces, air pollution, including volatile organic compounds, particulate matter, ozone, oxides of nitrogen and fugitive methane emissions.
There’s often large withdrawals of surface water. There can be groundwater impacts with chemicals and ending up in groundwater near these operations.
Importantly, these operations are very visible, not only is there truck traffic, but there’s odor and vibration and light and noise.
Many of these visible things can cause stress and people who live around these.
And so what’s important, as we think about health, is that we have a mix of exposures that can affect health in many ways.
And these can be cumulative and increase in their effects over time for both acute, that is, short occurrence, and then chronic health effects.
Multiple Peer-Reviewed Studies
And so, at this point there’s quite a few studies. We’ve heard from the prior speaker about all the different studies that have been done.
My group at Geisinger now has nine peer-reviewed publications on fracking and health in top scientific and medical journals. [Read more here.]
These are peer-reviewed, which means that it’s very difficult to pull a fast one on scientists because we have to respond to all of the comments that they provide to us after they review our manuscript before it is published.
The prior speaker spoke about distance, but when we look at fracking activity in communities, we’re not only evaluating the distance, we’re also evaluating the total number, the size of the wells in terms of the total depth and the gas production, the phase of the well development. And so it’s not just about proximity.
We’ve studied a range of common, severe, and impactful health outcomes across the lifespan at virtually all ages.
We’ve done both electronic health record-based studies and questionnaire-based studies.
In the electronic health records, we go into the electronic health records on millions of patients in the Geisinger system over 20 years, but only about 12 or 13 during this industry.
We’ve studied asthma exacerbations. We find out when people with asthma went to the emergency room and went to get hospitalized and figured out what was going on in terms of fracking at that time.
We’ve looked at hospitalizations for congestive heart failure, adverse birth outcomes, including preterm birth, high-risk pregnancy, and birth weight.
We’ve looked at mental health in pregnant women and mental health diagnosis and treatment in adolescents, all with electronic health records.
So we know the date. We know when medications were prescribed. We know when testing was done. We know when diagnoses were obtained and provided by healthcare providers.
We’ve also done questionnaire-based studies and looked at a variety of symptoms like the other studies you heard about and have published several papers on nasal and sinus and headache and depression symptoms.
Many of the findings of our studies have been found before us or replicated by other investigators in Pennsylvania and other states.
Finally, this industry has fugitive emissions of methane and the burning of gas releases carbon dioxide.
And finally, many of the resources from this industry are going into plastics production.
And so all of these have very significant impacts on climate change. And climate change is happening now, it’s affecting health now, and it’s affecting the health of Pennsylvanians now.
So this industry has local, regional, and global impacts on health. And I want to emphasize that our studies are of Pennsylvania residents.
And while Maryland and New York have prohibited this industry, the state with the most health studies has not. And that is Pennsylvania.
Should We Believe The Findings
So I was asked– is there enough evidence? And should we believe these findings?
I think we should believe these findings.
In epidemiology and in public health, we look at the body of evidence. And the body of evidence is large, growing, and consistent.
Many people ask us to prove whether this industry is causing these problems, but epidemiologic studies cannot prove anything. We look at the body of evidence.
Don’t forget that long after public health professionals concluded that cigarette smoking caused lung cancer, tobacco companies continued to claim that it had never been proven.
So this is just a common strategy used by industry to delay. And it is not a compelling reason not to act.
So why is the existing evidence compelling? Well, we have studies from many groups of independent investigators. We have studies using different study designs, including some that more formally evaluated causality using specific cause and effect frameworks.
There are studies from many parts of the United States, but as I said, most of the evidence is from Pennsylvania.
The studies that we have selected are biologically-plausible health outcomes where we study health outcomes that we do not expect could be affected by this industry.
We do not have to find anything, but when we pick outcomes that we believe could be, we do.
We find in our studies that as somebody’s value of their unconventional natural gas development activity metric goes up, the risk or severity of the health outcome goes up.
And in epidemiology, we call this a dose response relation. And this is very important to find.
We also really evaluate the robustness of our findings.
As I often say, epidemiologists find stuff and then we try to make it go away. We try to control for cigarette smoking, and we try to control for other things. And if it goes away, we tend not to believe it.
But all of our findings are very robust.
Finally, nothing else has changed in this region as rapidly as the fracking industry in the same time and places.
The industry criticizes our findings but offers no alternative explanation for how all of these various health outcomes could be caused by something else.
They have not offered any plausible alternatives. They just claim that there’s no proof of causation.
But there’s certainly enough evidence to act.
As we’ve heard from prior speakers, we should be protecting public health.
As I said, the best studies on health impacts have been from Pennsylvania. And Pennsylvania has not acted.
And I’m here to tell you that there is sufficient evidence to act now.
Key recommendations referred to by Dr. Schwartz in his testimony by the Environmental Health Project include–
1. Adopt a health-protective approach to shale gas development. Policy makers should halt or mitigate the risks to the community by preventing exposure to air and water contamination when there is uncertainty about its effects on residents, especially children, pregnant women, the elderly, and those with existing health conditions.
Primary consideration should be given to the people living within proximity to any shale gas facility, ensuring they are not exposed to levels of emissions harmful to themselves or their families.
2. Shift the burden of proof to industry and away from residents. Government agencies should require shale gas companies to disclose expected emissions to the public and to install monitoring equipment—the data from which should be made publicly available—to ensure that degradation of industry systems do not risk public health over time.
Agencies should establish such monitors and compliance of standards before granting permits. Further, agencies should appropriately classify waste streams based on the toxics they contain.
All waste must be tracked from cradle to grave and disposed in a fashion that prevents exposure to residents. Once operational, any company failing to comply with regulations and standards should lose its permits to operate.
3. Increase public participation in health decision making. People who live in proximity to shale gas development should be involved in decisions that affect their own health. This is especially true of those in underserved and underrepresented areas.
Government agencies should develop and maintain open channels of communication that allow residents to easily and without threat of retaliation share health information and harms related to shale gas development.
Departments of health should actively warn residents of the risks they face and provide advice to them and to physicians for how they can best protect themselves and others from exposure.
Departments of environmental protection should notify communities of any substantive changes to existing permits or permit applications, as well as any industry violations, so that residents and communities can better manage the associated health risks.
4. Fully fund and staff government agencies that protect public health. State departments of health and environmental protection should be adequately supported so that they can investigate and monitor the entire shale gas development process, from site preparation through waste treatment and sequestration.
Relying on industry to self-report emissions, waste, and health impacts does not provide adequate safeguards to public health.
5. Work toward a quick and just transition away from fossil fuels and toward renewable energies. Policy makers should take into account global and local health impacts, economic priorities, and environmental justice issues when making policy regarding shale gas development.
Fossil fuel extraction, transportation, processing, and consumption hastens the warming of the planet and exposes local residents and their families to numerous serious and documented health risks.
In addition to examining economic and social factors, a consideration of health impacts is central to any policy decision, especially when underserved and underrepresented communities are involved.
When that failed to make me become a quiet obedient Albertan, they lied in their 2012 brief filed in court (written by outside counsel Glenn Solomon; it’s against law society rules for lawyers to lie, accidentally or intentionally – but, Alberta lawyers lie, a lot, intentionally and get away it again and again with law society doing little but huff and puff), saying I was a terrorist, and thus I had no Charter rights so it was fine for my rights to be violated. Then Court of Queen’s Chief Justice Neil Wittmann wrote in his ruling there was “absolutely” no evidence I was a terrorist but punished me and rewarded AER, making me pay legal costs for the regulator violating my rights and further, lying about me to the court. When AER and the Alberta courts were unable to stop or silence me, Supreme Court of Canada J Rosalie Abella took the lies deep into Hell. She pulled facts out of her corrupt ass, changed AER’s calling me crazy, then criminal, then terrorist, to vexatious litigant – two years before I became a litigant. Miraculous ass-bound justice, Canada-style.
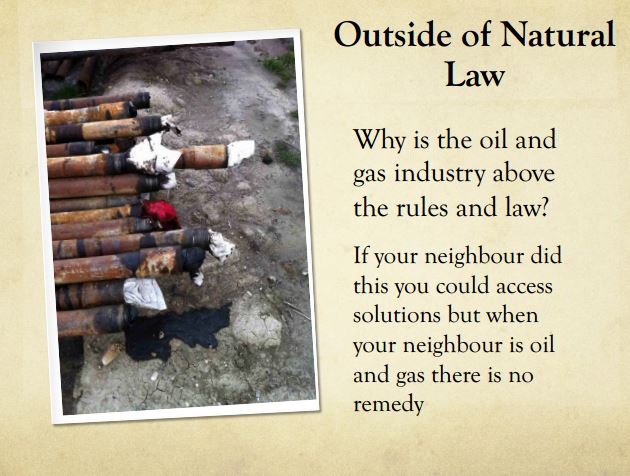
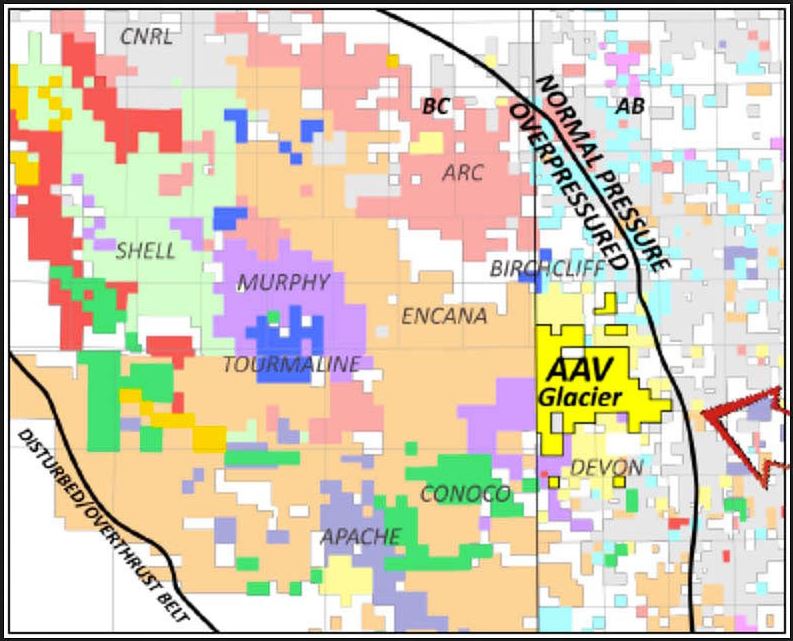
2001-onward: Encana/Ovintiv illegally frac’s drinking water aquifers at Rosebud Alberta, invades them also elsewhere in Canada and in Pavillion Wyoming and Silt Colorado:
2011:
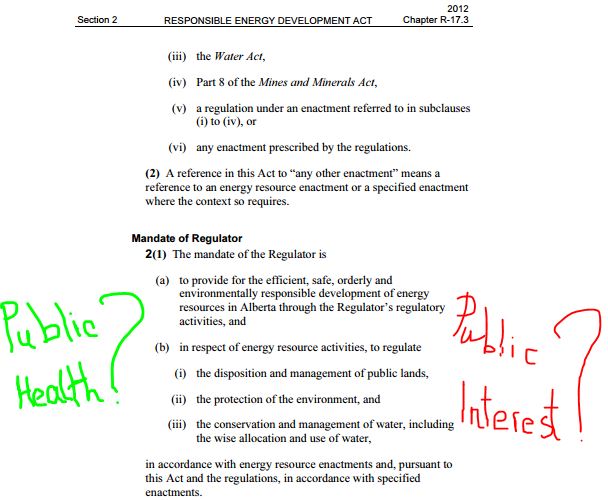
ERCB was the energy regulator in Alberta then, it was the EUB but when it got caught spying on innocent ordinary citizens, the gov’t changed it’s name to hide the growing scandal. After the Ernst lawsuit against the EUB, Alberta Environment and Encana went public, the gov’t changed it to AER, removing its public interest mandate.
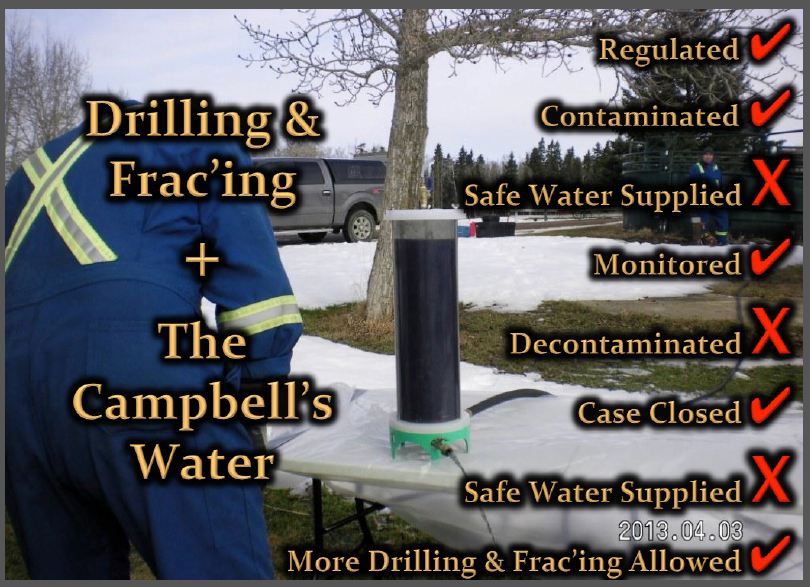
2013: AER slams the door shut on Shawn and Ronalie Campbell (their water was frac’d by Encana in 2005; isotopic fingerprinting by U of A matched ethane, propane, butane and pentane in their water to the company’s zones of production). Yes, that black stuff is their drinking water.
This website stores cookies on your computer. These cookies are used to provide a more personalized experience and to track your whereabouts around our website in compliance with the European General Data Protection Regulation. If you decide to to opt-out of any future tracking, a cookie will be setup in your browser to remember this choice for one year.