
“Neurological manifestations after COVID-19 may be multifaceted and long-lasting.”
“We believe long COVID results in an inflammatory response that may predispose patients to premature coronary artery disease, pulmonary hypertension, and valvular damage such as stenosis or regurgitation.”
@HarrySpoelstra CardioVascular Surgeon, international clinical research:
Need for awareness and surveillance of long-term post-COVID neurodegenerative disorders. A position paper from the neuroCOVID‐19 task force of the European Academy of Neurology
!!IMPORTANT WARNING in support of our longstanding call for caution!
“Neurological manifestations after COVID-19 may be multifaceted and long-lasting.”
“The associations of the neuropathological changes in the acute phase with subsequent neurodegeneration are HIGHLY LIKELY and the role of inflammation as an underlying mechanism is emerging.”
“An increase in the incidence of neurodegenerative diseases might be expected.”
“Awareness is particularly needed given that clinical manifestations months or years after SARS-CoV-2 infections may no longer be quoted as post-COVID symptoms, and hence, progressing pathologies at the community level may remain unnoticed.
!! Please taker this warning seriously, AVOID SARSCOV2!
Need for awareness and surveillance of long-term post-COVID neurodegenerative disorders. A position paper from the neuroCOVID‐19 task force of the European Academy of Neurology by Dániel Bereczki, Ádám Dénes, Filippo M. Boneschi, Tamar Akhvlediani, Francesco Cavallieri, Alessandra Fanciulli, Saša R. Filipović, Alla Guekht, Raimund Helbok, Sonja Hochmeister, Tim J. von Oertzen, Serefnur Özturk, Alberto Priori, Martin Rakusa, Barbara Willekens, Elena Moro & Johann Sellner on behalf of the NeuroCOVID-19 Task Force of the European Academy of Neurology, 6 May 2025
Journal of Neurology Volume 272, article number 380, (2025)
Abstract
Background
Neuropathological and clinical studies suggest that infection with SARS-CoV-2 may increase the long-term risk of neurodegeneration.
Methods
We provide a narrative overview of pathological and clinical observations justifying the implementation of a surveillance program to monitor changes in the incidence of neurodegenerative disorders in the years after COVID-19.
Results
Autopsy studies revealed diverse changes in the brain, including loss of vascular integrity, microthromboses, gliosis, demyelination, and neuronal- and glial injury and cell death, in both unvaccinated and vaccinated individuals irrespective of the severity of COVID-19.
Recent data suggest that microglia play an important role in sustained COVID-19-related inflammation, which contributes to the etiology initiating a neurodegenerative cascade, to the worsening of pre-existing neurodegenerative disease or to the acceleration of neurodegenerative processes. Histopathological data have been supported by neuroimaging, and epidemiological studies also suggested a higher risk for neurodegenerative diseases after COVID-19.
Conclusions
Due to the high prevalence of COVID-19 during the pandemic, healthcare systems should be aware of, and be prepared for a potential increase in the incidence of neurodegenerative diseases in the upcoming years. Strategies may include follow-up of well-described cohorts, analyses of outcomes in COVID-19-registries, nationwide surveillance programs using record-linkage of ICD-10 diagnoses, and comparing the incidence of neurodegenerative disorders in the post-pandemic periods to values of the pre-pandemic years. Awareness and active surveillance are particularly needed, because diverse clinical manifestations due to earlier SARS-CoV-2 infections may no longer be quoted as post-COVID-19 symptoms, and hence, increasing incidence of neurodegenerative pathologies at the community level may remain unnoticed.
***
@drseanmullen:
COVID AWARE + LONG COVID WARRIORS: Your doctor doesn’t believe you? THIS WILL HELP
Tired of being gaslighted by medical professionals who don’t understand #LongCovid? I’ve compiled ALL the scientific evidence into ONE printable document you can bring to appointments.
This 1-page letter contains:
- Critical references on brain, heart, and immune system damage
- Scientific proof of how COVID damages multiple organs
- Evidence that validates YOUR symptoms
- Key studies doctors need to see
Just print it double-sided and hand it to your doctor. Knowledge is power, especially when fighting for proper care.
Because NO ONE should have to fight to be believed while also fighting to recover.
MedicalGaslighting #LongCovidAwareness #ChronicIllness #PatientAdvocacy
Still Masked, Still Right: A Data-Driven Case for Vigilance by Sean P. Mullen, PhD, Associate Professor, Health and Kinesiology, Director, Exercise, Technology, and Cognition Lab University of Illinois Urbana-Champaign, May 7, 2025
This brief was prepared to support patients who continue to take precautions against SARS-CoV-2 and/or report symptoms that may be downplayed. The evidence summarized below reflects current peer-reviewed science on the effects of SARS-CoV-2 on the brain, immune system, cardiovascular system, and overall functioning—even after mild or asymptomatic infection.
1. SARS-CoV-2 is a vascular and neuroinvasive virus—not just a respiratory one.
▪ Neuroimaging data show measurable brain tissue loss, cognitive decline, and disrupted neural networks post-infection—even in non-hospitalized adults.1
▪ Cognitive deficits resembling IQ loss, attentional dysfunction, and memory decline are well-documented in both adults and children.2,3
▪ Viral particles have been found in the brain, vasculature, and bone marrow months after infection. 4,5,6
2. Damage occurs even after “mild” or asymptomatic infections.
▪ Studies confirm structural and functional brain changes after mild cases, particularly in areas responsible for memory, attention, and executive function.7,8
▪ Many individuals show signs of organ dysfunction (e.g., cardiovascular, renal) without overt symptoms—just as in hypertension or cancer before clinical presentation.9,10
3. SARS-CoV-2 impairs immune function—sometimes long-term.
▪ T-cell exhaustion, persistent inflammation, and immune dysregulation are well-documented months after infection.10-12
▪ Children also experience neutrophil dysfunction and inflammatory syndromes despite mild illness.13-15
4. Children are not spared their other organs.![]() BC’s Dr Bonnie Henry, social murderer extraordinaire, has much to answer for because of her lying to the public and parents especially, claiming kids don’t get COVID, don’t transmit it, or bring it home.
BC’s Dr Bonnie Henry, social murderer extraordinaire, has much to answer for because of her lying to the public and parents especially, claiming kids don’t get COVID, don’t transmit it, or bring it home.![]()
▪ A major cohort study of nearly 300,000 infected children showed increased risk of myocarditis, arrhythmias, thromboembolism, and heart failure months after infection.16
▪ Kidney dysfunction and neuropsychiatric manifestations have been reported in pediatric populations.17,18
5. Functional impairment is often invisible but real.
▪ Individuals may struggle with cognition, fatigue, sensory overload, or post-exertional malaise even if routine labs appear “normal” yet they may perform poorly at mental tasks or while operating heavy machinery, including driving19,20.
6. Masking and other protections are rational—not pathological.
▪ A person choosing to wear a high-quality mask, even when not ‘fitted’ in a clinical setting is applying layered, evidence-based risk reduction.21
▪ Avoiding repeat infections is not fear—it is a science-informed strategy to protect brain, heart, immune, and societal health. These are just facts.
This summary reflects peer-reviewed research from top-tier journals and global experts. For references and further reading, see reverse side.
References ![]() Refs are live linked there
Refs are live linked there![]()
1. Wood GK, Sargent BF, Ahmad ZU, et al. Posthospitalization COVID-19 cognitive deficits at 1 year are global and associated with elevated brain injury markers and gray matter volume reduction. Nat Med. Published online 2024. doi:10.1038/s41591-024-03309-8.
2. Douaud G, Lee S, Alfaro-Almagro F, et al. SARS-CoV-2 is associated with changes in brain structure in UK Biobank. Nature. 2022;604(7907):697-707. doi:10.1038/s41586-022-04569-5
3. Hampshire A, Azor A, Atchison C, et al. Cognition and memory after COVID-19 in a large community sample. N Engl J Med. 2024;390(9):806-818. doi:10.1056/NEJMoa2311330..
4. Monje M, Iwasaki A. The neurobiology of long COVID. Neuron. 2022;110(22):3484-3496.
doi:10.1016/j.neuron.2022.10.006.
5. Stein SR, Ramelli SC, Grazioli A, et al. SARS-CoV-2 infection and persistence in the human body and brain at autopsy.
Nature. 2022;612(7941):758-763. doi:10.1038/s41586-022-05542-y.
6. Rong Z, Mai H, Ebert G, et al. Persistence of spike protein at the skull-meninges-brain axis may contribute to the neurological sequelae of COVID-19. Cell Host Microbe. Published online November 29, 2024. doi:10.1016/j.chom.2024.11.007.
7. Samanci B, Ay U, Gezegen H, et al. Persistent neurocognitive deficits in long COVID: Evidence of structural changes and network abnormalities following mild infection. Cortex. 2025;187:98–110. doi:10.1016/j.cortex.2025.04.004
8. Xu E, Xie Y, Al-Aly Z. Long-term neurologic outcomes of COVID-19. Nat Med. 2022;28(12):2406-2415. doi:10.1038/s41591-022-02001-z.
9. Ewing AG, Salamon S, Pretorius E, et al. Review of organ damage from COVID and Long COVID: a disease with a spectrum of pathology. Med Rev. 2024;5(1):66-75. doi:10.1515/mr-2024-0030
10. Kubisiak A, Dabrowska A, Botwina P, et al. Remodeling of intracellular architecture during SARS-CoV-2 infection of human endothelium. Sci Rep. 2024;14:29784. doi:10.1038/s41598-024-80351-z.
11. Phetsouphanh C, Darley DR, Wilson DB, et al. Immunological dysfunction persists for 8 months following initial mild-to-moderate SARS-CoV-2 infection. Nat Immunol. 2022;23(2):210-216. doi:10.1038/s41590-021-01113-x.
12. Pedroso RB, Torres L, Ventura LA, et al. Rapid progression of CD8 and CD4 T cells to cellular exhaustion and senescence during SARS-CoV-2 infection. J Leukoc Biol. 2024;116(6):1385-1397. doi:10.1093/jleuko/qiae180.
13. Chou J, Thomas PG, Randolph AG. Immunology of SARS-CoV-2 infection in children. Nat Immunol. 2022;23(2):177-185. doi:10.1038/s41590-021-01123-9.
14. Bodansky A, Mettelman RC, Sabatino JJ Jr, et al; Overcoming COVID-19 Network Investigators. Molecular mimicry in multisystem inflammatory syndrome in children. Nature. 2024;632(8025):622-629. doi:10.1038/s41586-024-07722-4.
15. Kovács F, Posvai T, Zsáry E, et al. Long COVID syndrome in children: neutrophilic granulocyte dysfunction and its correlation with disease severity. Pediatr Res. Published online November 27, 2024. doi:10.1038/s41390-024-03731-1.
16. Zhang B, Thacker D, Zhou T, et al. Cardiovascular post-acute sequelae of SARS-CoV-2 in children and adolescents: cohort study using electronic health records. Nat Commun. 2025;16:3445. doi: 10.1038/s41467-025-56284-0
17. Li L, Zhou T, Lu Y, et al. Kidney function following COVID-19 in children and adolescents. JAMA Netw Open. 2025;8(4):e254129. doi:10.1001/jamanetworkopen.2025.4129
18. Ewing AG, Joffe D, Blitshteyn S, et al. Long COVID clinical evaluation, research, and impact on society: a global expert consensus. Ann Clin Microbiol Antimicrob. 2025;24(1):Article 793. doi:10.1186/s12941-025-00793-9
19. Erdik B, Homrich D. Driving under the cognitive influence of COVID-19: exploring the impact of acute SARS-CoV-2 infection on road safety. Neurology. 2024;103(7_Suppl_1):S46-S47. doi:10.1212/01.wnl.0001051276.37012.c2
20. Erdik B. Driving under viral impairment: Linking acute SARS-CoV-2 infections to elevated car crash risks. PLOS Glob
Public Health. 2025;5(4):e0004420. doi:10.1371/journal.pgph.0004420
21. Greenhalgh T, MacIntyre CR, Baker MG, et al. Masks and respirators for prevention of respiratory infections: a state of the science review. Clin Microbiol Rev. 2024;37(2):e00124-23. doi:10.1128/cmr.00124-23
Further Reading & Public Resources
• The Hidden Damage to the Immune System
• Why I Still Wear an N95 – A Doctor’s Perspective | Stuck in the Middle with Masking – Playing the Long Game
MORE RESOURCES TO HELP YOU NAVIGATE COVID PRECAUTIONS + LONG COVID
Coming soon: 1-pager on ‘Returning to Physical Activity’ (safe guidelines according to the best available evidence)
For explaining to others: Can’t find the right words for family/friends/coworkers? This letter helps them understand what you’re going through → https://uofi.box.com/s/wki3eb09dee3i29617lstxe6t2f034pk
For institutional advocacy: Originally for Mensa, this document has helped many secure accommodations from employers and event organizers → https://uofi.box.com/s/to7acbvjeh679fzvwimlgh4ovfdncqfx
Because NO ONE should have to fight to be believed while also fighting to recover.
MedicalGaslighting #LongCovidAwareness #ChronicIllness #PatientAdvocacy
@uht_fresh:
THIS informational document is EXCELLENT!!!!
I wish I had this letter to shove at HR when I was fighting for Reasonable Accommodation.
That letter should be helpful to many needing professional backup when it is sorely lacking.
Maybe a copy for @LongCLand?
***
@PutrinoLab:
Great to see this paper out, showing persistent heart and lung inflammation in people with #LongCOVID, but also highlighting once again that SARS-CoV-2 is a virus that profoundly affects vascular health and that every new infection can do damage.
Long COVID May Cause Long-Term Changes in the Heart and Lungs and May Lead to Cardiac and Pulmonary Diseases, Mount Sinai study suggests COVID-19 infection should be considered a risk factor for future cardiopulmonary conditions by Mount Sinai, May 6, 2025
New York, NY:
Patients suffering from long COVID may exhibit persistent inflammation in the heart and lungs for up to a year following SARS-CoV-2 infection—even when standard medical tests return normal results—potentially placing them at elevated risk for future cardiac and pulmonary conditions. These findings come from a new study conducted by researchers at the Icahn School of Medicine at Mount Sinai and published April 30, in the Journal of Nuclear Medicine.
The study, the largest of its kind using advanced PET/MRI imaging, discovered significant abnormalities in cardiovascular and pulmonary tissues, as well as altered levels of circulating immune-regulating proteins, in long COVID patients. These abnormalities could serve as early warning signs of diseases such as heart failure, valvular heart disease, and pulmonary hypertension.
“Long COVID has emerged as a major public health challenge, and the long-term sequelae remain largely undefined,” says corresponding author Maria G. Trivieri, MD, PhD, Associate Professor of Medicine (Cardiology), and Diagnostic, Molecular and Interventional Radiology at the Icahn School of Medicine. “This study brings us closer to understanding how SARS-CoV-2 affects the heart and lungs over time. We believe long COVID results in an inflammatory response that may predispose patients to premature coronary artery disease, pulmonary hypertension, and valvular damage such as stenosis or regurgitation.”
“Since 2020, we have been publishing work showing that even mild or asymptomatic COVID infections can have serious cardiovascular consequences, even in previously fit and healthy individuals,” says David Putrino, PhD, the Nash Family Director of Mount Sinai’s Cohen Center for Recovery from Complex Chronic Illness. “This paper provides more data to highlight that SARS-CoV-2 is a virus that profoundly affects vascular health and that every new infection can do damage. Infection prevention is crucial.”
Researchers studied 100 adult Mount Sinai patients who had a confirmed COVID-19 infection between December 2020 and July 2021 and were experiencing persistent cardiopulmonary symptoms. Most of these patients had no previous diagnosis of cardiovascular disease. About 300 days after their initial infection, 91 participants underwent hybrid 18F-fluorodeoxyglucose positron emission tomography combined with magnetic resonance imaging (PET/MRI), an advanced imaging method that simultaneously detects structural and metabolic abnormalities. Among those scanned, 52 patients—representing 57 percent—demonstrated evidence of inflammation affecting the heart muscle, pericardium (the thin sac that surrounds the heart), heart valves, particularly the mitral valve, and the aortic and pulmonary blood vessels. In several cases, more than one of these regions was affected.
The PET/MRI scans revealed myocardial (heart muscle) abnormalities in 22 participants, characterized by scarring and thickening of the tissue, similar to findings of myocarditis or cardiomyopathy. Pericardial involvement was seen in 20 patients, indicating either inflammation or effusion, a buildup of fluid. Inflammation near the mitral valve was identified in 10 participants, and vascular inflammation involving the aorta or pulmonary arteries was observed in 28 participants. All abnormalities were associated with persistent symptoms such as chest pain, fatigue, and shortness of breath.
In parallel, researchers performed plasma protein analysis, which showed abnormal patterns in key biomarkers that regulate inflammation and immune signaling. These findings correlated with the imaging abnormalities, providing molecular-level confirmation of persistent inflammation.
To further validate the results, a control group of nine individuals with confirmed prior COVID-19 infection but no lingering cardiopulmonary symptoms was studied between March and October 2023. These controls underwent the same imaging and blood testing and did not exhibit the inflammatory changes observed in the symptomatic long COVID cohort.
“We found a range of cardiopulmonary inflammatory patterns, backed by abnormal protein profiles,” Dr. Trivieri says. “These insights could have far-reaching implications for diagnosis and surveillance. If patients experience lingering symptoms such as shortness of breath, they should consult a physician for further evaluation. Our results should also raise awareness among clinicians to consider a patient’s COVID history and evaluate persistent symptoms more thoroughly.”
Zahi Fayad, PhD, senior author of the study and Director of the Biomedical Engineering and Imaging Institute at the Icahn School of Medicine at Mount Sinai, emphasized the broader impact of these findings. “This study highlights the unique power of hybrid PET/MRI imaging to uncover hidden disease processes in long COVID patients,” Dr. Fayad says. “These findings should change how we approach care and surveillance—not only recognizing SARS-CoV-2 as a potential long-term cardiovascular risk factor, but also integrating molecular imaging into post-COVID evaluation protocols. We now have objective evidence that can guide earlier detection and potentially prevent future cardiopulmonary events.”
The Mount Sinai team continues to follow this patient cohort to assess long-term outcomes and is exploring whether these imaging and biomarker patterns can help predict who is most at risk for developing chronic cardiovascular or pulmonary disease after COVID-19.
Mount Sinai Is a World Leader in Cardiology and Heart Surgery
Mount Sinai Fuster Heart Hospital at The Mount Sinai Hospital ranks No. 4 nationally for cardiology, heart, and vascular surgery, according to /U.S. News & World Report®./It also ranks No. 1 in New York and No. 6 globally according to /Newsweek’s/“The World’s Best Specialized Hospitals.”
It is part of Mount Sinai Health System, which is New York City’s largest academic medical system, encompassing sevenhospitals, a leading medical school, and a vast network of ambulatory practices throughout the greater New York region. We advance medicine and health through unrivaled education and translational research and discovery to deliver care that is the safest, highest-quality, most accessible and equitable, and the best value of any health system in the nation. The Health System includes approximately 9,000 primary and specialty care physicians; 11 free-standing joint-venture centers throughout the five boroughs of New York City, Westchester, Long Island, and Florida; and 45multidisciplinary research, educational, and clinical institutes. Hospitals within the Health System are consistently ranked by /Newsweek/’s® “The World’s Best Smart Hospitals” and by /U.S. News & World Report/’s® “Best Hospitals” and “Best Children’s Hospitals.” The Mount Sinai Hospital is on the /U.S. News & World Report/‘s® “Best Hospitals” Honor Roll for 2024-2025.
For more information, visit https://www.mountsinai.org
Prevalence of Persistent Cardiovascular and Pulmonary Abnormalities on PET/MRI and DECT Imaging in Long COVID Patients by Maria Giovanna Trivieri, Ana Devesa, Philip M. Robson, Sonali Bose, Busra Cangut, Steve Liao, Audrey Kaufman, Renata Pyzik, Valentin Fauveau, Jamie Wood, Aaron Shpiner, Edwin Yoo, Sarayu Huang, Claudia Calcagno, Venkatesh Mani, Sahityasri Thapi, Johanna Contreras, Kai Nie, Seunghee Kim-Schulze, Sacha Gnjatic, Miriam Merad, Munir Ghesani, David Putrino, Adam Jacobi, Donna Mancini, Charles Powell and Zahi A. Fayad
Journal of Nuclear Medicine April 2025, jnumed.124.268980; DOI: https://doi.org/10.2967/jnumed.124.268980
Abstract
The objective of this study is to describe the prevalence of inflammatory cardiopulmonary findings in a prospective cohort of long coronavirus disease (LC) patients. Methods: Subjects with a history of coronavirus disease 2019 infection, persistent cardiopulmonary symptoms 9–12 mo after initial infection, and a clinical assessment compatible with LC underwent cardiopulmonary 18F-FDG PET/MRI, dual-energy CT (DECT) of the lungs, and plasma protein analysis (subgroup). A control group that included subjects with a history of acute severe acute respiratory syndrome coronavirus 2 infection but without cardiopulmonary symptoms at recruitment was also characterized. Results: Ninety-eight patients (median age, 48.5 y; 47% men) were enrolled. The most common LC symptom was shortness of breath (80%), and 27% of participants were hospitalized. Of the subjects, 90% presented abnormalities in DECT, with 67% and 59% of participants demonstrating pulmonary infiltrates and abnormal perfusion, respectively. PET/MRI was abnormal for 57% of subjects: 24% showed cardiac involvement suggestive of myocarditis, 22% presented uptake reminiscent of pericarditis, 11% showed periannular uptake, and 30% showed vascular uptake (aortic or pulmonary). There was no myocardial, pericardial, periannular, or pulmonary uptake on the PET/MRI scans of the control group (n = 9). Analysis of plasma protein concentrations showed significant differences between the LC and the control groups. Lastly, the plasma protein profile was significantly different among LC patients with abnormal and normal PET/MRI. Conclusion: In LC subjects evaluated up to a year after coronavirus disease 2019 infection, our results indicate a high prevalence of abnormalities on PET/MRI and DECT, as well as significant differences in the peripheral biomarker profile, which might warrant further monitoring to exclude the development of complications such as pulmonary hypertension and valvular disease.
Footnotes
- Published online Apr. 30, 2025.
- © 2025 by the Society of Nuclear Medicine and Molecular Imaging.
***
@HarrySpoelstra May 4:
‘These findings indicate that even mild COVID-19 can result in persistent neurocognitive deficits, structural brain alterations, and functional network abnormalities, both in individuals with and without brain fog.’
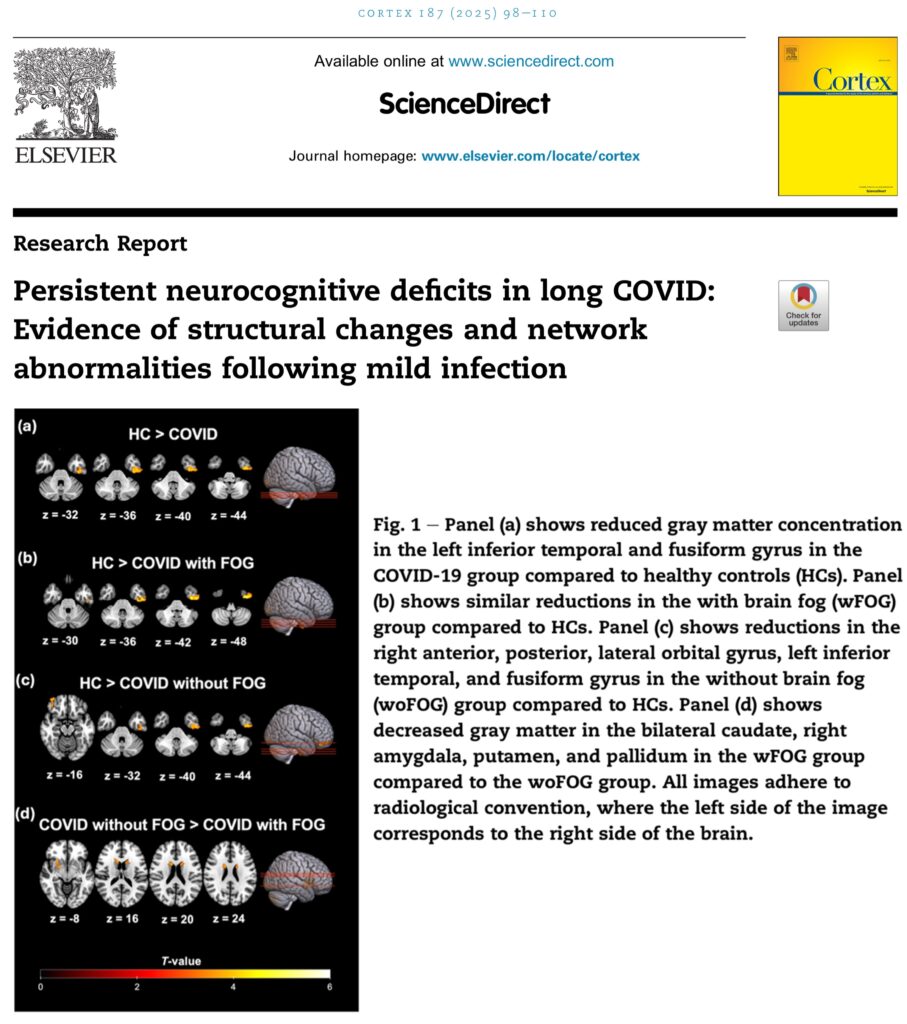
Research Report Persistent neurocognitive deficits in long COVID: Evidence of structural changes and network abnormalities following mild infection by Bedia Samanci, Ulaş Ay, Haşim Gezegen, Sanem Sultan Yörük, Alpay Medetalibeyoğlu, Elif Kurt, Erdi Şahin, Faruk Uğur Doğan, Mehmet Barbüroğlu, Başar Bilgiç, Haşmet Hanağası, Hakan Gürvit, June 2025, Cortex, Volume 187, June 2025, Pages 98-110
https://doi.org/10.1016/j.cortex.2025.04.004Get rights and content
Abstract
This study aimed to investigate the neurocognitive deficits, structural brain alterations, and network abnormalities in individuals who had a mild SARS-CoV-2 infection, with and without brain fog, as a symptom of long COVID. A cross-sectional study was conducted involving 75 participants, categorized into three groups: 24 healthy controls (HCs), 26 COVID-19 survivors without brain fog (woFOG), and 25 with brain fog (wFOG). Neuropsychological assessments included the Free and Cued Selective Reminding Test (FCSRT) and Addenbrooke’s Cognitive Examination–Revised (ACE-R). Structural and functional brain alterations were examined using voxel-based morphometry (VBM) and resting-state functional MRI (rs-fMRI). The wFOG group exhibited significant cognitive impairments, particularly in delayed free recall, attention, memory, and visuospatial skills, compared to both the woFOG and HC groups. Structural MRI analyses revealed reduced gray matter concentrations (GMC) in the left inferior temporal gyrus, left fusiform gyrus, and right orbital gyri in both COVID-19 groups relative to HCs. Additionally, the wFOG group exhibited further GMC reductions in the bilateral caudate nuclei, right putamen/pallidum, and amygdala compared to the woFOG group. rs-fMRI analyses demonstrated altered connectivity patterns in COVID-19 survivors, characterized by increased connectivity in the default mode network and visual networks, alongside decreased connectivity in the dorsal attention network. These findings indicate that even mild COVID-19 can result in persistent neurocognitive deficits, structural brain alterations, and functional network abnormalities, both in individuals with and without brain fog. The observed changes highlight the importance of long-term monitoring and targeted interventions to address potential cognitive and neurological consequences of long COVID.
@BensenHsu:
Breakdown of the paper:
The study aimed to investigate the neurocognitive deficits, structural brain alterations, and network abnormalities in individuals who had a mild SARS-CoV-2 infection, with and without brain fog, as a symptom of long COVID.
The group with brain fog showed significant cognitive impairments, particularly in delayed free recall, attention, memory, and visuospatial skills, compared to the other groups. Structural MRI revealed reduced gray matter concentrations in regions involved in memory and attention, with further reductions in the brain fog group. Resting-state fMRI showed altered connectivity patterns in COVID-19 survivors, with increased connectivity in the default mode network and visual networks, and decreased connectivity in the dorsal attention network.
***
@elisaperego78 May 4:
COVID-19 infection can cause long-lasting structural damage to the esophagus, thereby potentially contributing to gastric problems in #LongCovid, such as acid reflux
@HarrySpoelstra:
Acute COVID-19 and LongCOVID syndrome – molecular implications for therapeutic strategies – review
Fascinating yet grim review on long COVID: SARS-CoV-2 manipulates our body at the molecular level.
LongCOVID syndrome:
LCS problem have focused on describing the immunologic, molecular, and morphologic changes in the organs or tissues that are damaged or dysregulated, but initial pathobiochemical and molecular changes in cellular metabolism that lead to the observed LC end-effects are often forgotten.
Four main alternatives can be considered as the reason for LCS
1. COVID-19 activates multiple autoimmune diseases
2. Activation of other active chronic infections
3. Sars-Cov-2 still persisted in the cells despite negative tests:
“The mounting body of evidence indicates the presence of SARS-CoV-2 RNA and protein in a broad spectrum of tissue types, collected weeks or months after the onset of acute SARS-CoV-2 infection. The viral RNA or protein has been identified in the majority of organs and tissues, including the liver, stomach, tonsils, gallbladder, and lungs. The preponderance of evidence for the existence of a SARS-CoV-2 reservoir in individuals with LCS stems from three sources: tissue biopsy studies, studies of SARS-CoV-2 proteins in plasma and studies using features of the adaptive immune response to infer the presence of a SARS-CoV-2 reservoir in tissues.”
4. Molecular basis for the LongCOVID syndrome caused by SARS-CoV-2 persistence.(fig)
Metabolic alterations generated by SARS-CoV-2:
- Upregulation of the angiotensin 1 receptor
- Upregulation of calcium stress by SARS-CoV-2
- Creating potassium/calcium channels by ORF3a
- Reticuloendoplasmic stress caused by ORF3a and M proteins
- Loss of endothelial monolayer integrity caused by Spike protein
- Neuraminidase activity of the spike protein
- SARS-CoV-2 and mitochondria
- Disrupting the mitochondria by ORFs
- Inhibition of Nrf2 by SARS-CoV-2
- Activation of HIF-1α
- Inhibition of autophagy by ORF3a, NSP6, ORF7a, NSP15, M and E proteins
- Upregulating the inflammation
- Inhibition of Interferon production
Conclusion:
‘Analysis of the feedback loops shows that the regulatory system is extremely complex. The multitude of positive feedback loops suggests that treatment strategies with a single drug acting on a single therapeutic pathway or transcription factor have little chance of bringing the patient out of hyperinflammatory or chronic state, as the remaining active positive feedback loops continue to drive inflammation and oxidative stress, leading all the time, but only slightly weaker, to the destruction of the system.
!! The deeper we explore, the more intricate it gets—hardly encouraging, as we’re still searching!
PREVENTION remains our STRONGEST DEFENSE!

Acute COVID-19 and LongCOVID syndrome – molecular implications for therapeutic strategies – review by Krzysztof Piotr Michalak, Amelia Zofia Michalak and Alicja Brenk-Krakowska, April 16, 2025
REVIEW article
Front. Immunol., 16 April 2025
Sec. Molecular Innate Immunity
Volume 16 – 2025 | https://doi.org/10.3389/fimmu.2025.1582783
Severe Acute Respiratory Syndrome Coronavirus 2 (SARS-CoV-2) has been recognized not only for its acute effects but also for its ability to cause LongCOVID Syndrome (LCS), a condition characterized by persistent symptoms affecting multiple organ systems. This review examines the molecular and immunological mechanisms underlying LCS, with a particular focus on autophagy inhibition, chronic inflammation, oxidative, nitrosative and calcium stress, viral persistence and autoimmunology. Potential pathophysiological mechanisms involved in LCS include (1) autoimmune activation, (2) latent viral persistence, where SARS-CoV-2 continues to influence host metabolism, (3) reactivation of latent pathogens such as Epstein-Barr virus (EBV) or cytomegalovirus (CMV), exacerbating immune and metabolic dysregulation, and (4) possible persistent metabolic and inflammatory dysregulation, where the body fails to restore post-infection homeostasis. The manipulation of cellular pathways by SARS-CoV-2 proteins is a critical aspect of the virus’ ability to evade immune clearance and establish long-term dysfunction. Viral proteins such as NSP13, ORF3a and ORF8 have been shown to disrupt autophagy, thereby impairing viral clearance and promoting immune evasion. In addition, mitochondrial dysfunction, dysregulated calcium signaling, oxidative stress, chronic HIF-1α activation and Nrf2 inhibition create a self-sustaining inflammatory feedback loop that contributes to tissue damage and persistent symptoms. Therefore understanding the molecular basis of LCS is critical for the development of effective therapeutic strategies. Targeting autophagy and Nrf2 activation, glycolysis inhibition, and restoration calcium homeostasis may provide novel strategies to mitigate the long-term consequences of SARS-CoV-2 infection. Future research should focus on personalized therapeutic interventions based on the dominant molecular perturbations in individual patients.
***
@HarrySpoelstra May 2:
The Effects of COVID-19 on Voice
Interesting article on the possible long-term damage to your vocal cords, of special interest to people needing their voice professionally!
Most studies report the prevalence of dysphonia in COVID-19 infection to be 25%–28% with varying
For patients who experience dysphonia during COVID infection, 70% of these dysphonic patients may have long-lasting voice sequelae
Etiology of Voice Changes due to COVID-19 are multifactorial in etiology, but one can be Vagus Nerve related……sounds familiar @DavidJoffe64?
“The effect of COVID-19 on the voice is complex, multifaceted, and still being defined. Dysphonia may be an initial indication of infection, may persist throughout the illness and recovery, and may even remain long-term.”
“Treatment focuses on the underlying cause and can include voice therapy as well as surgical intervention.”
“For laryngeal surgeons, a thorough subjective and objective analysis is crucial.”
“A detailed history of the disease progression along with videolaryngoscopic and acoustic voice assessment is essential to capture the wide range of potential diagnoses.”
” Videostroboscopy and acoustic voice analysis are encouraged for all patients presenting with dysphonia.”
“A multidisciplinary approach involving otolaryngologists, speech-language pathologists, and pulmonologists helps address the complex and multifactorial etiologies of COVID-19 dysphonia.”
“Lastly, treatments focusing on anti-inflammatory and anti-reflux measures have shown to improve vocal outcomes, while frequent surgical intervention to maintain airway patency may have deleterious effects but are nonetheless necessary.”
!!This has intrigued me ever since I had my first C19: “Your voice has changed” dixit my wife!
C19 keeps on giving……..grrrrrrrr. Avoid C19, especially reinfections!!!!
The Effects of COVID-19 on Voice by Mausumi Syamal, 30 April 2025, Wiley Research
https://doi.org/10.1002/wjo2.70012
ABSTRACT
The COVID-19 pandemic had profound effects on vocal health, impacting both infected individuals, professional voice users and essential workers. The objective of this paper was to explore the multifaceted nature of dysphonia associated with COVID-19, arising from both direct and indirect consequences of the pandemic. Prevalence rates of dysphonia among COVID-19 patients range widely from 25% to 79%, with significant underreporting. Factors contributing to voice changes include laryngeal inflammation, respiratory function impairment, treatment-related interventions, and increased vocal strain from masking and virtual communication. Professional voice users, such as teachers and singers, experienced unique challenges, including increased voice fatigue and apprehension regarding aerosol transmission during singing. For the voice clinician, videolaryngoscopic examination remains the critical tool for capturing the broad landscape of diagnoses that can range from inflammation to surgically emergent airway stenoses. Innovations with voice also emerged, utilizing artificial intelligence voice analysis for COVID-19 detection. Overall, understanding the relationship between COVID-19 and voice health is crucial for appropriate diagnosis and treatment of dysphonic patients. Continued research is necessary to further delineate the long-term implications and optimal treatment approaches for those affected.
@Mike_Honey_:
Was listening to an actor’s podcast today – his usual rich deep voice in the pre-recorded segments contrasted with his current scratchy, rasping almost gaspy delivery.
Notable coughing by him off-mic, throughout.
“But when we return [so and so] tells how they have managed [such and such] – since the pandemic”