Lyme disease increases risk for multiple gynecological conditions by Paige S. Hansen Colburn, Grace Blacker, Sarah Galloway, Qingying Feng, Prasanna S. Padmanabham, Guido Pisani, Brandon T. Lee, Grace Loeser, Monika W Perez, Kunzan Liu, Jade Kuan, Emelia von Saltza, Satu Strausz, Lisa M. Mattei, Sophie VanderWeele, George R. Nahass, Amie Kitjasateanphun, Rangarajan Bharadwaj, Hari-Hara SK Potula, Maia Atzmon Shoham, Finngen, Victoria L. Mascetti, Eric Gars, Hanna M Ollila, Kaylon L. Bruner-Tran, Irving Weissman, Sixian You, Beth Pollack, and Linda Griffith, March 6, 2025, BMJ Yale
doi: https://doi.org/10.1101/2025.03.03.25323258
This article is a preprint and has not been peer-reviewed.
Abstract
Lyme disease (LD) is an illness caused by the spirochete Borrelia burgdorferi (B. burgdorferi). Borrelia is known to disseminate through organs, including the skin, joints, spinal cord, bladder, and heart, leading to Lyme arthritis, neuroborreliosis, and Lyme carditis. While previous studies have investigated the impact of LD on pregnancy in both mice and humans and have found the presence of B. burgdorferi in the uterus of mice, we studied the impact of LD on the non-pregnant female reproductive tract. We use a mouse model for LD and find an ongoing and severe infection of the reproductive tract of female mice, which persists up to 15-months post-inoculation. This infection results in uterine glandular cysts and endometrial hyperplasia as well as vaginal epithelial thickening, polymorphonuclear and mononuclear cell epithelial infiltration, and epithelial desquamation into the vaginal lumen. Strikingly, we find that age has an impact on the extent of gynecologic pathology such that aged female mice (1-year old) that are reproductively senescent have more gynecologic pathology with infection compared to young mice (15-weeks old) when infected for the same length of time. Using large-scale electronic healthcare record data, we report that LD additionally results in increased infection-associated risk of menorrhagia (1.5-fold), miscarriage (1.62-fold), uterine fibroids (1.42-fold), and endometriosis (1.93-fold). Underreporting of gynecological outcomes is pervasive throughout many different infectious diseases, and LD-associated gynecological pathologies may have been similarly underappreciated in the field. This work suggests that further study of the female reproductive tract and the effects of B. burgdorferi infection therein will help clarify and expand the knowledge of myriad LD outcomes.
Chronic Lyme Shows Women’s Bodies Need Specialized Research, Lyme can persist in the uterus for 1 year by Anthony J Leonardi, MBBS, PhD, Mar 13, 2025
A new preprint from the MIT lab of Michal Tal highlights the critical need for specialized research funding to address the unique physiological and immunological differences in women’s bodies. Biological sex plays a profound role in how diseases manifest, progress, and respond to treatment, yet medical research has historically prioritized male subjects, leaving significant gaps in our understanding of women’s health. These disparities are not merely academic—they translate into real-world consequences, such as delayed diagnoses, inadequate treatments, and poorer outcomes for women. To bridge this gap, we must advocate for targeted funding that recognizes women’s bodies as distinct systems deserving of rigorous scientific inquiry.
One striking example of this need is the recent discovery that Lyme disease, caused by the bacterium Borrelia burgdorferi, can persist in the uterus for over a year, leading to vaginal and uterine complications. This finding underscores how pathogens may interact differently with female reproductive tissues, potentially due to hormonal influences or immune responses unique to women. The female reproductive tract is an immunologically complex environment, balancing tolerance (e.g., for pregnancy) with defense against infection. Persistent Lyme in the uterus suggests that women may harbor chronic infections in ways that men do not, contributing to under-recognized symptoms like pelvic pain, abnormal bleeding, or infertility. Without dedicated research funding, these sex-specific manifestations remain poorly understood, leaving women vulnerable to misdiagnosis and ineffective care.Similarly, the phenomenon of long COVID highlights how immune system differences between sexes can disproportionately burden women. Studies indicate that women are more likely to develop long COVID, experiencing persistent symptoms such as fatigue, brain fog, and autoimmune-like conditions. This disparity may stem from women’s more robust immune responses, driven by genetic factors and hormonal influences like estrogen, which enhance immune activity but may also predispose to immune dysregulation. In contrast, men often experience more severe acute COVID-19, while women bear the brunt of chronic sequelae. This pattern suggests that women’s immune systems handle pathogens differently over time, necessitating research into sex-specific mechanisms and therapies.
The implications of these examples extend beyond individual diseases to the broader framework of public health. Women’s health issues, particularly those tied to chronic or misunderstood conditions like Lyme disease and long COVID, impose significant societal costs—lost productivity, increased healthcare utilization, and diminished quality of life. Yet, funding for women’s health research remains a fraction of what is allocated to more generalized (and often male-centric) studies. By investing in specialized research, we can uncover the molecular and immunological underpinnings of these disparities, paving the way for precision medicine tailored to women. This approach not only benefits patients but also strengthens public health systems by addressing a historically neglected population.
In conclusion, the distinct biology of women’s bodies demands a paradigm shift in medical research funding. Discoveries like the persistence of Lyme in the uterus and the disproportionate impact of long COVID on women reveal the urgent need to prioritize sex-specific studies. As an immunologist and public health advocate, I see this as a moral and scientific imperative: we cannot achieve equitable healthcare without understanding how diseases uniquely affect half the population. By channeling resources into women’s health research, we can illuminate these differences, improve clinical outcomes, and honor the complexity of the female immune system. The time for action is now—women’s lives depend on it.
![]()
Refer also to:
![]() If only the pro rape/abuse propagandists had written things happening as in this cartoon when they wrote their misogynistic bible:
If only the pro rape/abuse propagandists had written things happening as in this cartoon when they wrote their misogynistic bible:![]()
Denise Bella @denisebella:
Unbelievable. What year is it? 1950?
Clara Loiseau@ClaraLoiseauJDM:
Ça m’étonne presque qu’il y ait UNE femme!
West Coast Lass@Liv_F:
Let the mansplaining of women’s health begin. Sigh.
Debbie@ironbow:
Aww, all those white men certainly will have the expertise on women’s health, won’t they?
Trish Paton@trishpaton:
Robert Kitchen, good lord the last person needed on any health committee that’s not about preserving white christian conservative male power is Kitchen. …
@TheoAnonis:
Evangelical Christianity is a cancer.
Conservatism is a cancer.
Both act to forcefully replace decency and virtue with violence and hatred.
![]() Canadian Con Politicos, including their leader, vile racist misogynistic Trump-worshipping Pierre Poilievre, currently are all anti women’s choice. Disgusting inhumane anti-health prejudice in these old white con men. Typical that anti-women men are on a women’s health committee, likely ordered so by women-hating rape religions; there’s nothing worse for women’s health than religious men, notably those that yak Pro Life:
Canadian Con Politicos, including their leader, vile racist misogynistic Trump-worshipping Pierre Poilievre, currently are all anti women’s choice. Disgusting inhumane anti-health prejudice in these old white con men. Typical that anti-women men are on a women’s health committee, likely ordered so by women-hating rape religions; there’s nothing worse for women’s health than religious men, notably those that yak Pro Life:![]()
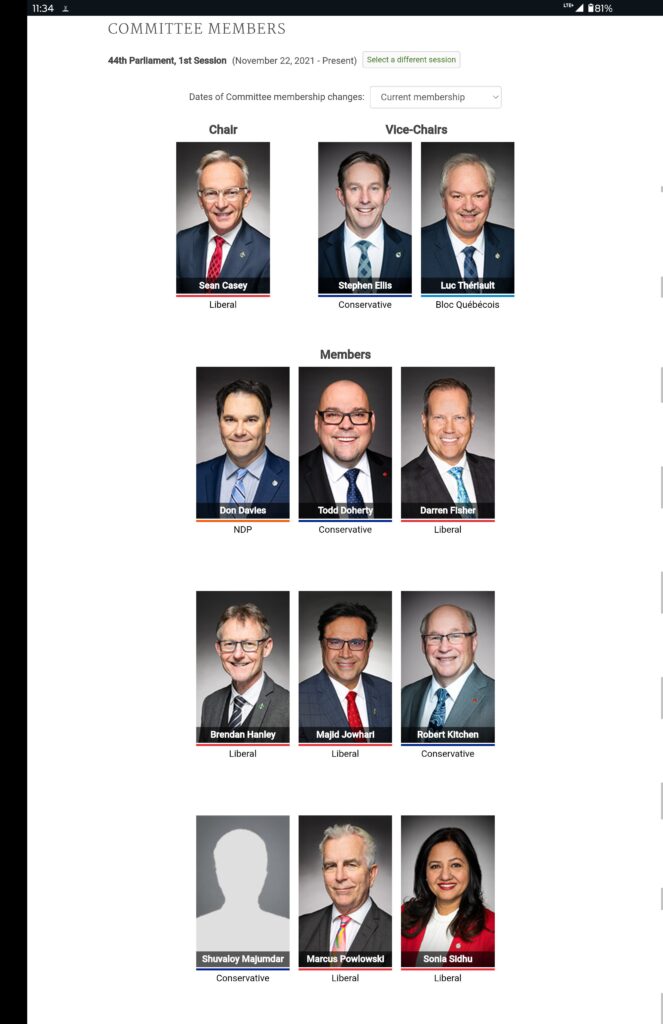
![]() Too funny, the old white men above look like the old white men below:
Too funny, the old white men above look like the old white men below:![]()